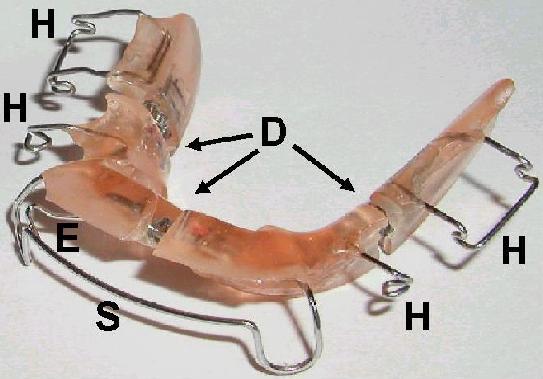
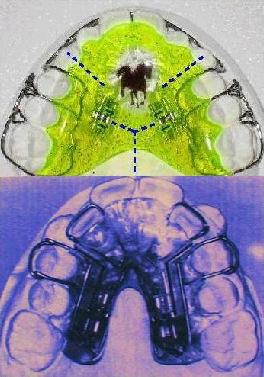
Common plate appliances (here for lower jaw)
These
two similar appliances exemplify the formerly widespread
„active plate appliance“. It was not just an „expander“ to
gain space, but allowed for dental straightening almost at the
same time – if constructed and handled properly! H =
anchoring clasps, D = expansion screws (which in fact
require growth to work properly), here even in 2 directions E =
spring for a tooth correction, shaped according to the desired
movement, S = labial arch (a common element).
Most
of the following appliances are based on this, but developped
further.
In the second specimen, the anchoring clasps at the
rear are slightly simpler, but the front is equipped more
generously with protrusion springs for tidying up crowded teeth.
Find examples of full treatments with plates in the „case examples“ chapter. Hints for distinctive applications of Crozat and plate appliances are there in the sub-chapter about classical Crozat treatment.
DNA
appliance ® (no image or central link here)
means
day-
and nighttime appliance: for
children, teenagers and adults, 12
- 16 /24h lead painlessly
to
success. DNA as well alludes to the theory behind it, the
utilization of epigenetic
jaw and arch development, including the nasal pathways, so that it
cures also certain cases of snoring.
This plate appliance is for controlled expansion in all directions, to fulfil what is genetically possible. It is made with patented, pre-shaped parts that require no or little adjustment. First publication was in 2009 as a lighter wireframe appliance, suitable for appropriate cases.
However,
this appliance seems to have no class-III type, that means, for
patients with lower jaw before upper (what is for the lower jaw,
honestly spoken, not a problem of underdevelopment).
To
track down further removable appliances and treatment by
orthopedic exercises, search also for „Integrative
orthodontics“.


Wrong: how a blocked canine tooth was kept trapped
This
is a typical example of a poorly designed plate appliance.
Treatment started in late mixed dentition, where the gap for one
of the cuspids (canine or eye teeth) had much narrowed. But
instead of re-expanding it little by little, the positions of the
adjacent teeth were retained by this plate.
Since it has the
screw elements in wrong positions, it wasted 2 precious years of
growth and made the case severe. An attempt to obtain a second
opinion in time failed, because the visited orthodontist was one
of those who make all patients first wait until all milk teeth are
gone. This strategy aggravates all cases more or less, which
increases the profit for the orthodontist as well as the pain and
damage that the late treatment does to the patients. The patient
here was menaced by a common package of orthodontic extortion:
mutilating extractions, or headgear, or expensive, but hampering
large fixed installations (pendulum, distal jet) - and each of
these combined with fixed bracket braces.
The
rarer specialists of gentle treatment offered mainly Crozat
appliances (see below), which are however rarely covered
by public health insurance.

Plate utilities: crossed wire fingers to close frontal gap; pro-loop
Interspaced
incisors are not crooked in a medical sense. Nevertheless, these
little gaps may waste space which will later lack for the larger
canine teeth (eye teeth, cuspids).
Plate appliances for
„gappers“ can be equipped with adjustable wire fingers to
close up the teeth. If, moreover, an expansion screw is used, this
can close up wire fingers by the same distance, if they are
embedded crosswise in the halves of the plate, as shown
here.
Screwed expansion also stretches and flattens a common
frontal arch wire spring, as shown below. This is helpful if
incisors stick out.
Against the opposite case, if incisors grow
inward (retruded) of the arch line, plate appliances can be
equipped with protrusion springs, either one by one (see above
under „Common plate appliances“), or in the shape of an inner
arch with loops.
In the specimen for interceptive treatment
shown here, this element should stretch back when the plate is
expanded. However, if it would also be embedded with crossed ends,
then expanding the plate should bend it in the desired forward
direction. Such a plate design, out of standard materials, may
replace a specialized component: the robust, but sometimes bulky
3-way screw of Bertoni (see below, for T-segmented plate
expanders).
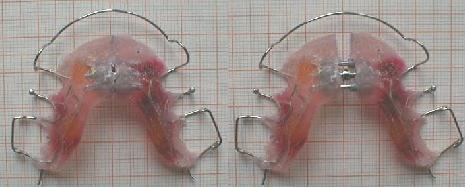

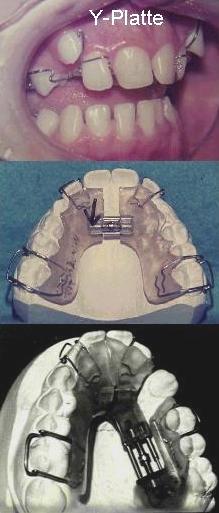
Plate with additional clasps (Voss plate): expansion, distalization, vampire canine teeth
To
develop a narrow jaw or a crowding of side teeth into a healthy
situation by means of a plate, this appliance requires screwed
segments in the right positions. Moreover, it needs sufficient
anchorage for efficient force
transmission. Additional clasps at both sides of the screw prevent
the plate from lifting off when it is screwed onward,
to avoid that it loses its proper fit and that most of its force falls flat.
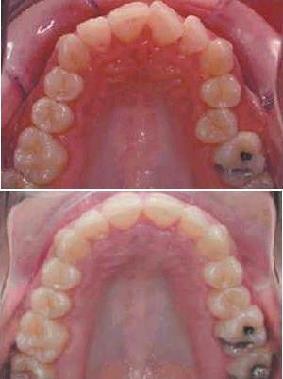
In
this sense, the first photo shows a typical vampire canine teeth
(eye teeth, cuspids) situation. The
narrowed gaps have already been re-gained. This appears to be a Y
plate (see below) with additional clasps on the 2s and 4s here,
and with guide wires for the cuspids which are now free to grow
down.
The next photo shows a used plate expander with
additional clasps on the 2s. It had expanded the maxilla by
approximately 5 mm even in this stage with no more milk teeth
left. Also the green specimen under Plates
for one-sided expansion against
single-sided crossbite has additional clasps.
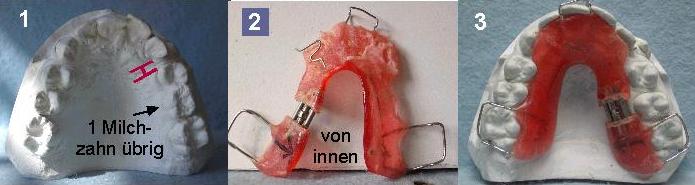
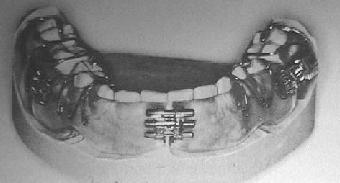
The
b/w photo shows a successful re-distalization of 3 teeth which had migrated forward.
This plate has a further screw for simultaneous expansion, which
was not used here. Teeth often move forward when milk teeth are
destroyed before their successors are ripe, and narrow the
gap as is exemplified in the
sequence below: the gap for the canine tooth is narrowed to 1/3!
Just 1 milk molar is left, but when it falls, it will provide
another 2 mm of space.
2 wire elements support this plate in
the incisor region. It successfully regained the
lacking space by its backward screwed (distal) segment. It was
provided with a lining of fresh plastic material during this, to
re-establish the neat fit which generally degrades when screwed
segments are used to greater extent. This treatment was
accomplished by an activator which had additional guide elements
for the growing cuspid as well as for the bicuspids which appeared
rotated due to excess of space.
No lobby acts for proven and economic techniques like this one. In contrast, manufacturers of countless fixed distalizers and „bone piercing“ (micro-implantat anchorage) engage reputable speakers for courses to promote these risky and forced techniques, which endanger children as well as adults.

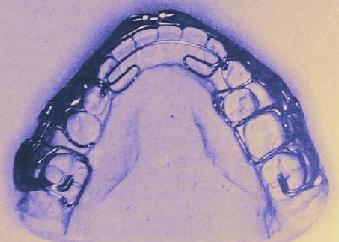
Y plates, Z plates, Bertoni plates
Due
to their large roots, cuspids (canine oe eye teeth) are important
teeth, but often develop later than both their neighbors. Space
can lack for them in case of insufficient jaw growth or premature
loss of milk teeth. Then they often grow off-site, mostly before,
rarer behind the main row of teeth.
Treatment
would be easier when not waiting so long.
Y
and Z plates use 2 common screws to regain this space. Narrowed
gaps can nicely be expanded by the plastic ends of the screwed
segments. These have to be shortened little by little when the
tooth grows in or is being aligned.
The Y-shaped segmentation
of the colourful upper specimen causes expansion as well as
stretching of the jaw. This is a light case, whereas the harder
case in the mouth photo in vampire
canine teeth above obviously also
uses a Y or Z plate: screw elements inside of the narrowed gaps
had already re-gained them by expansion and stretching.
The
following specimens (yellow and violet-from-b/w) have their screws
more distally placed. They finger into the cuspid position by a
Z-shaped 3-segmentation of the plate. By their rather sagittal
direction, the gap is opened mainly by stretching and
distalization.
Y and Z plates
differ less in the lower jaw (pink specimen). The screws can be
placed more or less frontally there.
The
indication for the Y plate overlaps with that of the more recent
Bertoni screw (3-way-screw). The green plate shown below contains
it, and moreover 2 distal screws, so that this plate has 5
segments! Nevertheless it is not bulky, and is even more
versatile than a Y or Z plate to shape the dental arch.
In
addition, it is equipped to derotate the canine teeth,
which are rotated by narrowing, already while the space for them
is under way to be recovered. Such details make the difference
between high-value plates for removable treatment and plates
which are just preparing for fixed braces. 3- or 4-way screw
elements also exist for lower jaw plates.
Such plates as shown here were proven for treatment of children and, by taking some more time, also for teenagers. Nowadays, they fall into oblivion, irrespective that they offer a way out of the frequent bad business which is exemplified above under Wrong .. canine tooth had to stay trapped: only treatment with extractions or with a headgear was offered there, or sometimes with more expensive, hindering fixed appliances under the palate (Pendulum, Distal jet), or even piercing mini implants (micro screws, micro pins) through the flesh into the bone, which imposes a considerable risk of persistent bone inflammations to the patient.



Molar distalization by screwed segments: (pre-prosthetic) adult treatment; impacted canine teeth
A)
Special element included: double screw with 2 independent segments
in series:
The
symmetrical blue plate contains this element on both sides. All 4
premolars lack in this adult upper jaw: 2 had been sacrified for
orthodontic treatment long ago, and 2 were destroyed more
recently. These latter should now be replaced, but the molar teeth
have already migrated forward and narrowed the gaps too much.
Therefore, the screwed segments should recover sufficient gaps.
The enlarged image with the red arrows shows that the front
segment is to shift towards the fixed position of the screw heads,
while the rear segment is to shift away from it. A jagged anchor
for this long element can be seen embedded in the plastic behind
the incisors.
B)
2 small standard expansion screws, aligned in series: In the
next, 25-yr case, the canine teeth stayed impacted in the
jawbone.
Sufficient space was created for them with the violet
distal plate shown here and a subsequent one, by pushing teeth
forward and others backward. The big molar teeth had to be pushed
individually, each with its own screwed segment of the plate, 1 on
the right and 2 on the left hand side here. Thus, the
second-but-last molar can be shifted individually, if the more
frontal screw is opened and the rear screw closed by the same
amount.
After enough space was provided, one canine tooth grew
in by itself, whereas the other had to be cut free and pulled out
slowly, by glueing a hook to it and connecting it with a rubber
band to a corresponding hook at the appliance. A formerly common
procedure, to which Crozat appliances (see below) are also
suitable.
The
lower plate shown on the right side is similarly built, to help
the canine tooth out of crowding. Photos from top to bottom are
taken for illustration (in treatment, both segments should rather
be alternated in smaller steps):
1) at start, no length
expansion
2) rear segment length expanded (distalize molars 6
and 7)
3) middle segment length expanded, rear segment
equivalently re-contracted (push back 4 and 5 and shift a frontal
wire along which contacts the canine).
For better guidance,
these both segments have plastic-fitted clasps.


Crozat appliances
are the oldest system of removable braces, invented
and developped to mastery in the 1920ies, before plastic era. Wire
elements of different thicknesses were soldered together to light,
hygienic appliances which are well-suited for full-time wear,
in particular for adult and pre-prosthetic treatment, and if teeth
or gums have already damages.
Experts performed full treatments
with these appliances, not restricted to simple cases, since they
can widen and lengthen the arches and correct individual teeth. A
limited expansion of the upper jaw is still possible in adults
– slowly, but with these appliances with little discomfort.
Inspite of all the orthodontic „late cases“ (= teenagers and adults),
this gentle and proven method is hardly reported anywhere in the mass media.
Rather, orthodontic implants are systematically disseminated
in congress-filling manner as a high-profit invasive technique,
but endanger the patient with persistent
bone inflammations (see below under „Less discomfortable additives..“ for more about it).
Find Crozat cases and details of this method in the „case examples“
chapter.

Hybrid type and upgraded Crozats
Hybrids between Crozat and plate appliances can be built economically from common materials without soldering or welding. E.g. the blue lightweight spring expander in the upper photo. There, small plastic wings bear common clasps (anchors) and are connected by a thicker wire spring. Even prefabricated parts which are intended for fixed use (lingual arch, palatal bar, quad helix ...) could be adapted for this, to make their use friendlier.
Normal Crozats have just 2 clasps, which are in the molar region. Because they were originally intended to give teeth just stimuli in the desired directions, and to leave them otherwise free to find their anatomically functional positions. Of course, Crozats can be built with more clasps, but that could hamper this original intention. In some cases it cannot be foreseen if 2 clasps would be enough. The lower photo shows an upgraded Crozat. Before, its anchorage had turned out to be insufficient. Occlusal extensions were also desired to treat a crossbite. They were added out of plastic material, and additional clasps embedded in them.


Lightweight expanders with screw or spring instead of quadhelix or other fixed expanders
Removable expanders can be built such that they do not hinder speech, because leaving the frontal palate free, and that they are little visible when worn. In the upper specimen, plastic snaps over the side teeth instead of clasps. This is also suited for slow expansion in permanent dentition (upper jaw still expandable up to 4-6 mm). It could also be made by thermoforming of plastic sheet. For children whose side teeth are changing, on the other hand, ordinary clasps are preferable.
Continuous force can either be provided by a screw with an included spring,
which is a specialized part, or by simple wire loops in spring
expanders as shown below with various clasps. The strength or
thickness of their spring can be varied, and also the position
where it leaves the plastic wings. For details on this, also for
the lower jaw, see Lightweight
prototypes chapter.
Even more than 4 -5 mm width can be gained in children
by removable expanders, with no need of splitting the palatal
suture, fixed quad helix or other cruel treatment. Such widespread
forced methods neclect loving care (find victims´ reports in the
„Less disturbing kinds“-chapter), but are favoured by
orthodontic manufacturers of many profitable prefabricated parts.
These force the dentitions of individual humans into uniform
shape.
If the molars are too conical or not yet fully erupted, so that these appliances fit too loosely, then tiny white attachments could be glued to them, which are now widespread in aligner orthodontics. In contrast to bands or brackets, they neither hurt the flesh, nor hamper cleaning these teeth far inside the mouth. The appliance would snap in firmly on these attachments, like an aligner splint (see below).

Plates for single-sided expansion (indeed!)
with
an approximate force distribution of 2/3 to 1/3, to correct a
one-sided crossbite that has already grown-in. For one-sided
crossbite in early state (muscular crossbite), a simple expansion
plate would often be sufficient (force distribution of 1/2 to
1/2).
A solution from old literature, the 1/4 – 3/4 divided
activator (double decker appliance), would be larger scale. The
fixed, pre-fabricated quad helix, in contrast, disturbs
swallowing, speech and chewing (see examples in the „less
disturbing kinds...“ chapter). Moreover, it has more relapses
than expansion plates have.
Both specimens shown here
are asymmetrically divided.
The green belonged to a 8-yr girl
who was menaced with rapid palatal
expansion (RPE) elsewhere. To unlock the wrong occlusion,
this plate extends over the side teeth. Additional clasps
assure a good grip, and the large expansion screw bears an
included spring to deliver a continuous force. Simultaneously, 3
protrusion springs are to widen the frontal arch, and a finger
spring is to re-gain the narrowed space for a growing canine
tooth.
The yellow specimen, which could also be equipped with
further elements, has a simple, big expansion screw and another
solution for a more continuous force delivery: the contact zone to
the teeth which are in crossbite consists of silicone rubber.

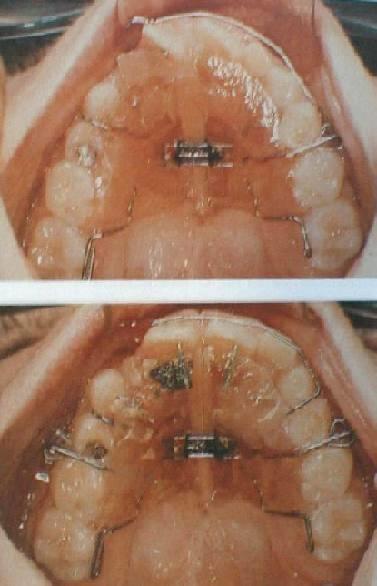
Plate with spring bolt screws
By
use of a reamer, the tiny spring-bolt screws can be
inserted later into a plate appliance, e.g. if changing teeth
appear too much inward.
In the example here, a young
cleft-palate patient with 45° twisted incisors profits from
skillful removable treatment. The screws act from inside and the
frontal wire from outside to untwist these teeth. Note also that
the expansion screw is already expanded by about 5 mm!
In the
following picture, the left one of the frontal screws has been
re-inserted, to re-adapt its direction to the proceeding
alignment.
This
example demonstrates that even a cleft-palate child is not condemned
to palatal splitting and other painful fixed stuff,
if the treatment is continuous.
Find more details in the „expl.
of cases“ chapter.

Plates equipped with silicone rubber for „complicated“ tooth correction
If sufficient space has been provided, this rational
technique can correct teeth which are in the row but nevertheless
not straight, that means tilted (around 3 axes possible).
This
appliance is mainly a plate, with a rigid body and clasps (and
screws would also be possible). It should provide a framework
around those (tilted) teeth which are to align. On the plaster
model, these are then cut out and re-fixed in aligned positions
(setup / aligner techniques). Silicone rubber is molded around
them onto the outer framework and the distant inner plate border.
Such
plates are smaller than the common elastic „positioners“,
which are mainly used when fixed braces gave no good result, but
can also be applied independently.
Moreover, such a plate would
allow larger alignments / untwistings by modification:
stepwise alignment of the plaster model and subsequent renewal of
just the silicone rubber parts, which is easy.

2 more examples for silicone rubber bearing plates and splints: 1 fine and 1 wide alignment by W. Paulus.
Thermoformed splint for fine
correction of lower incisors, manufacture: First,
a soft spacer (with the blue stripes here) is molded over the
teeth of the original plaster model which are to align. The larger
the required corrections are, the thicker should be this. It is
cut to size and positioned on the model before the final, hard
splint is molded. That is cut to shape, and the spacer
discarded.
Next, a set-up of these teeth is done. Silicone
rubber is filled around them into the void of the splint which was
created by the spacer.
Plate with silicone rubber
for derotation of upper incisors at larger scale, an
ecomonic solution: First, the silicone presses the
teeth only there where larger movements are needed. The other
regions of these teeth on the corrected plaster model are waxed
out. This allows the silicone of the first run of this plate to
expand sidewards, when squeezing frontally as desired.
Depending
if the silicone has point contact or full contact to these teeth,
it will move them rather tipping or rather bodily. The plate can
moreover use screwed segments.
For its second run, the same
set-up model can be re-used. But now, all void is stuffed with
silicone, no more wax. Note well that it acts from both sides
here: the frontal wire before the incisors is modified with a
plastic shield, which bears also silicone inside.


Less discomfortable additives for fixed braces
Many
add-on parts for US style multibracket techniques
pay little attention to patient
comfort, because the patient, especially if a child, has no other
choice anyway. In addition, they hamper oral hygiene.
Later on,
the profitable international orthodontic business began to spread
further orthodontic armament in form of little mini implants (mini
pin, micro screw, mini screw, ...), which are pierced through the
flesh into the bone, for all type of better fixation of fixed
braces. Since they create a highway for bacteria into the bone,
where inflammations are difficult to cure, their unneccessary use
endangers adults and children. In contrast, they are completely
useless for removable techniques! But nevertheless, removables have
largely been abandonned.
Solutions
with less discomfort or danger are
obvious to those who are
familiar with removable techniques. For
single jaw treatment, no functional, but just plate
appliance technique can already help a lot. The images show a
speech-friendly, frontally open design of such an add-on plate,
and 2 solutions to snap it in: silicone
rubber to fixed buttons, or ball head clasps and outer grips for
removal. Common
orthodontic
tasks to apply it:
-Maintain
jaw width or position of last molars:
simple blank plate to wear at night or part-time. Instead of head
gear, lip bumper, nance appliance, palatal arch or other
disturbing stuff.
-Expansion:
screw, fan screw or spring expander (find more about this under
Lightweight
prototypes). Instead of quad
helix or splitting the palatal suture (for these, see victims´
reports in the „less
disturbing kinds of braces“
chapter).
-Protrusion of
incisors: plate with protrusion springs / screws instead of
disturbing lingual arches.
-Distalization
(backward shift) of molars: segmented
plate with distal screws, instead of headgear, lip bumper,
pendulum, distal-jet or other fixed instruments.
Concerning bite
correction and vertical deviations (deep bite, open bite),
prefabricated functional trainers are available, also such which
are compatible with multibracket appliances (T4B = trainer for
braces).
1) Class II overjet, also with increased overbite
(deep bite), can be corrected by sustained use of such trainers
for 1 – 3 years, instead of hampering Herbst appliances or other
bulky, unhygienic fixed parts.
2) More rapidly, a covered or
deep bite can be levelled out painlessly. The required vertical
forces are easily provided by biting on the trainer, instead of
fixed bite blocks which extremely hamper any mastication (and
subsequent digestion).
Apart
from the T4B, which resembles the
Muscle force Jaw shaper in shape (find instructions under Kaukraft
Kiefer-Former), but has grooves for fixed
braces, a thicker fixed-compatible trainer for covered bite is
available. In contrast, the covered-bite type of the Jaw shaper
allows the patient to keep an arch shape which is somewhat more
tapering than standard.


Lower exterior plate (buccal plate), e.g. for gap closure of a missing tooth
This appliance wears comfortably because without
plastic parts inside. It is described in literature only for the
lower jaw and has advantage for straightening inward tilted teeth
and for gap closure with a traction screw. E.g. for those 5% of
people whose premolars in position 5-below are not formed, if
their respective milk molars could not be preserved. The coloured
specimen is for demonstration.
Even nowadays it is told with commercial interest that this task would
require fixed braces to perform properly. But look in the case
reports
for successful removable treatments of such gaps. Spontaneous gap
narrowing by forward migration of the molars should be allowed
before fitting an appliance. Moderate speed when screwing or light
force when using springs (also Crozat appliances would work here)
are crucial for a tilt-free gap closure.
The monochrome views show a
specimen with an additional space creating screw between the
crowded tooth 5 and 6 here on the right, and a traction screw to
close a little gap on the opposite site.
A further application
would be the contraction of the lower front e.g. if it had been
expanded by tongue habits. With a frontal traction screw, and with
elastic silicone joints in the canine region, such an appliance
would contract the front, but not the whole arch.

Extrusion (elongation) of teeth / use of „shelves“ (tiny attachments)
To
close an open bite after growth has finished, and if it has not
just developped by muscular imbalance,
the respective teeth need grips to apply a force in extruding
direction (the image shows a dummy). But no need to make the grips
broader than required to pose a spring wire on them. Such tiny,
tooth-coloured „attachments“ do not irritate, nor hamper
cleaning. They are common in active splint treatment (see below),
for teeth which can otherwise not be grabbed sufficiently to
direct the desired force to them.
Here, the attachments give a grip to the surrounding spring of a
speech-friendly constructed open plate, so that its extrusion
force can be transmitted. This principle can be transferred to
extrude side teeth if required, and the plate can bear further
elements e.g. an expansion screw. Compare
with the discomfort of a common extrusion method: rubber bands
stretched between brackets or buttons in upper and lower
jaw.
Attachments
can also be used to improve anchoring clasps in difficult cases
e.g. when teeth are not fully erupted.

Intrusion (= pressing too long teeth more into the bone)
The
specimen shown here is intended for rather „cosmetic“
intrusion of the incisors. More often, re-intrusion of single side
teeth which have grown too long is required medically in
pre-prosthetic treatment.
Here, removable appliances are hygienic, especially for patients
who have gum disease.
Intrusion plates need good anchorage at
all other teeth, or extensions which allow to transmit the force
of biting down just to the teeth which should be intruded. When
anchoring teeth lack, also in children who lost many milk teeth at
once, one-piece appliances could be a better choice, e.g.
prefabricated trainers like the Muscle force Jaw shaper (see
Kaukraft
Kiefer-Former).
Active orthodontic splints, e.g. Invisalign or hand-crafted aligners
are
rather for permanent dentition and are continuously developped
further. They are no budget method, but comparison
of their price between several systems often pays, or even between
doctors offering the same system.
A set of many thin transparent aligner splints is generated, each of
which is some 0.2 mm correcter than the previous. Adults should
wear each aligner full-time for 2 weeks. Part-time wear will
prolong the treatment, but may be straightforward for
teenagers.
Some gain of space for crowded teeth is possible by
narrowing (stripping, slicing) the teeth, as has been done in this
example. In cases of open bite, little tooth-coloured attachments
can be included, similar as in Extrusion
(elongation) of teeth.
A combination of hard and softer splint materials can be helpful,
because under continuous force, orthodontic movements proceed
rapidly in the first 14 days and then slow down because the
surrounding tissue exhausts. Certain dental laboratories provide
hard-and-soft either as compound aligners, or as hard and soft
aligners to wear in turns. Both would improve the recovery of the
surrounding tissue from orthodontic strain, and thus make the
treatment more comfortable and nevertheless fast.
See link list (in German) under „ALIGNER (Korrekturschienen)“ for recommendable international suppliers.

Plate with tongue attracting element
Tongue malfunctions can cause teeth / jaw
disorders. Speech training can help more or
less. The most violent method of tongue correction are fixed
spikes!
In sharp contrast, this „comfortable-feeling“
appliance mimicks the morphology of the frontal palate by thin
silicone rubber, to give the tongue an almost natural surrounding
around a little hole,
which is placed to attract the tip of the tongue to its correct
position.
Such a plate could perform further development and
alignment at the same time, e.g. with screws. If the incisors were
tilted forward („protruded“) by tongue thrusting, they can be
pushed back by tightening the frontal arch wire. For this, the rim
of the plate has to be shortened there, of course.
From
old text Headgear Plate:
attaching a headgear to a removable plate spreads its heavy
force much wider than the usual fixation to the first molars,
which are menaced with root damage then (pain is always a
warning!). Besides, some kinds of coupled plates or function
regulators have similar effect as the headgear, but offer
additional features for further tasks. Be
aware that the headgear is historically old and primitive.