Alternatives
to „torture instrument“ style and risky braces
Last
update: 06.10.2011
|
IMPORTANT
HEADER: Lobbyism by orthodontic societies and
manufacturers ignores and suppresses the indigenous European
techniques of jaw orthopedics and orthodontics, which mainly base
on individually hand-crafted, removable appliances with
utilization of growth.
It seems nowadays that these budget
methods of treatment, even if well-proven for over 50 years, are
hardly taught anywhere, in sharp contrast to all these highly
profitable fixed techniques and their progresses. These are
excellent to tie patients, often children, to their users. They
impose many more risks and costs on them than removables would
do.
Since the common multibracket braces („traintracks“)
lack the hard body which all removables have, a choice of
additional parts and appliances exists to support this technology.
But these reduce the life quality of their victims further and are
theme of this chapter, following below.
On the other hand, I
know practices which flourish by mastery of full treatment with
well-taylored removables as formerly, not just with these reduced
auxiliaries for fixed braces. Because treatment with removables
requires a practice much less time and costs than „fixed“
treatment.
|
INTRO:
this overview cannot account for all special
cases and exotic alternatives. For reasons of copyright I cannot show
a complete horror cabinet here (who will lend his photographs for use
as bad examples?), but
www.madsen.de/pages/jugendliche.htm
shows a pretty collection.
Contradictions between his and my text are due to differing fields of
interest.
It
has to be emphasized that orthodontic „torture
instruments“ and gentler alternatives are often tools of
entirely different systems of orthodontics / jaw orthopedics,
which have developped separately with no contact to each other. Often
they are poorly compatible with each other. Even the age and sequence
of treatment differ: rather a sequence of fast single-task steps
there, rather a slow and earlier begun multi-tasking here. One can
imagine which way is less painful and bears lower risks.
Braces
that make both systems better compatible could be engineered (1
example in chapter Gentle braces A). However, this would
require good knowledge of both fixed and removable treatment systems.
All
following braces types except the headgears are fixed appliances of
„non-compliance therapy“. In this concept, children are not
even asked if they would be willing to wear a removable voluntarily.
This forcible concept has its root in the frequent boycott of
headgears and facial masks, and ignores completely that other jaw
orthopedic systems (plate appliances, functionals) exist elsewhere in
the world which do not require such extra-oral appliances!
Nevertheless the non-compliance therapy is even exported to countries
where such systems were well-established formerly.
Most
orthodontists do not know the full possibilities of removable
braces. It remains the task of parents with some diplomacy to point
their orthodontists towards these.
LATE
SEQUELAE ?
The technical facilities of remodeling dental arches
and jaws to a great extent by means of fixed braces and / or
headgears of any type may appear fascinating and profitable. But the
greater this artificial remodeling is, and it is especially high
after extraction of teeth, the higher is the danger of mismatch to
the individual skull shape and circuits of jaw functions. In addition
to the pain during treatment, which indicates damage of the roots
(reversible or irreversible), the everyday little damages caused by
the created mismatch are repaired by the young body, but no more when
aging (compare with backbone or knee pain appearing). A cluster of 6
victims from 2 sources (France, Germany, same time) is in the
appendix. Extractions for braces have gained ground in these
countries and meanwhile are not medically justified in over 60% of
these cases in Germany. In Great Britain, the situation seems
even worse, see www.orthodontic-outrage.com
!
The replacement of
individual by „industrialized“ orthodontic treatment, which
often neglects the benefit of utilizing growth, so that childrens´
and adults´ treatments can be performed in the same way, seems
to have caused these mindless mutilations.
Any further growth of 8- or 10-yr old children is trampled on when
pulling them new, healthy teeth. They are psychically traumatized,
and their dental arches then often distorted by „train tracks“
to unnatural-looking, tapering „mouse (or rabbit) jaws“, in
addition to narrowing the space in the nose and for the tongue, and
to the above-mentioned functional risks.
Even
without accounting for late sequelae, our former European
jaw-orthopedic care of children was more economic. Carefully designed
functional, plate or lightweight removables guided and enhanced jaw
growth and directed individual teeth to their positions. If some
crowding remains, or for adult patients, some space can be gained by
narrowing (slicing) the teeth.
Increased overjet and overbite, as
the horizontal distance and the vertical overlap of upper and lower
incisors are termed, are often caused by a too much backward position
of the lower jaw. In children, this can be healed by activators and
other appliances as shown in the Gentle braces
B chapter, even in cases with long face (vertical facial
growth), who are considered more difficult than those with broad
faces.
But the medical
mainstream is governed to bring profit to the business, not to the
people.
 OVERVIEW:
OVERVIEW:
All
following are fixed to metal bands which are cemented around the 6s
(first molar teeth, appear with 6 years). Some are also fixed to
other teeth. This increases the danger of caries at these huge,
important teeth, where interstitial caries can appear 10 – 20
years later. Since caries danger increases with duration, it is
especially high if the bands are already placed when the milk molars
start changing and remain in the mouth for many years while the
permanent dentition is straightened with a bracket appliance. By this
stepwise build-up of fixed appliances, doctors also tie little
patients to their practices.
1.a)
lingual arch (lower jaw), palatinal arch
= palatinal bow = palatal bar =
TPA (upper jaw).
Thick wires along inner side of teeth or palate,
1.b) Nance appliance with additional
little, slightly speech-hindering plastic platelet.
These upper appliances disturb when sucking sweets or pills.
2 victims´ reports in the appendix.
Purpose:
to keep the molars in place while teeth before them change (children)
or while gaps are closed with bracket appliances there. The palatinal
arch also allows slight expansion or serves to maintain jaw width
during use of headgears (2.) or after
„rapid palatal expansion“ (4.) or to derotate the connected
molars.
Alternatives:
almost any kind of removable appliance! 2 kinds especially for
derotation, see case examples chapter.
1.c)
quad helix, quadhelix: has additional windings
(helices) for purpose of expansion, which make it
bigger and much more disturbing, see victims´ report below.
CAUTION, this cheap part is applied quite
often today, even to small children from 3 years on (see photo in
milk dentition)!
Alternatives:
simple removable expansion plates, or improved ones with 2 directions
of force (Bertoni screw/ Y plate / „cases“>
transversal and sagittal expansion). Expansion springs for
more comfortable
wear („Lightweight
prototypes“ chapter, even prefabricated upper and lower spring
wires can be provided with clasps for removal),
Crozat, integral effect in Fränkel´s function regulators
or in „chewing gum effect“ appliances (chapter
Gentle braces B, „case examples“>
Bimler, „Weitere Info“ in natural jaw orthopedics).
1.d)
lip bumper (mainly for lower jaw): thick wire,
often wavy or plastic-coated. Entirely fixed or to be inserted into
fixed holders (like a headgear).
Purpose: mainly
stimulation of frontal jaw growth when space is lacking for the front
teeth (children), further like purpose 1.a).
Alternatives:
apart from plate appliances with 2-directional screw or with several
screws („cases“> transversal and
sagittal expansion) and from special types of functionals
(chapter Gentle
braces B),
„Lightweight prototypes“ chapter
shows fully removable lip shield appliances, which
offer further possibilities for adjustment.
 2
extra-oral forces (2.a)
headgear) were invented long
time before screwed plate appliances, and before functional jaw
orthopedics (mainly double-deckers = 1 piece for both jaws) was
discovered! In contrast to working with growth by these,
headgears often require additional braces to achieve a proper
matching of upper and lower teeth. The roots and surrounding tissues
of the molars to which headgears are connected are endangered by its
large force, which is indicated by pain as in the victim´s
report below. Headgears also disturb sleeping in side or belly
position. Even a harmful sideward shift of the connected molar teeth
already occurred, caused by sleeping on the side!
2
extra-oral forces (2.a)
headgear) were invented long
time before screwed plate appliances, and before functional jaw
orthopedics (mainly double-deckers = 1 piece for both jaws) was
discovered! In contrast to working with growth by these,
headgears often require additional braces to achieve a proper
matching of upper and lower teeth. The roots and surrounding tissues
of the molars to which headgears are connected are endangered by its
large force, which is indicated by pain as in the victim´s
report below. Headgears also disturb sleeping in side or belly
position. Even a harmful sideward shift of the connected molar teeth
already occurred, caused by sleeping on the side!
Purpose
1
(children):
reduce the forward growth of the upper jaw.
More recently,
headgears are also used coupled to double deckers, to „speed
them up“. By this, patients are faster prepared for installation
of subsequent „traintracks“ (bracket braces).
Alternatives:
for overjet with the lower jaw lying back, almost any in chapter
Gentle braces B
is appropriate. For overjet without fault of the lower jaw, not only
activators of „high“ shape can be used, but excessive
growth of the upper jaw is reported to be normalized by Fränkel´s
function regulators 1 or 2 (more: „Weitere
Info“ subchapters) or by bite jumper plates
e.g. of „Pro-Stab“
type, which moreover allow for time-saving
simultaneous alignment of teeth and of jaws (more: chapter
„case examples“).
Purpose
2 (teenagers and adults): distalize molars (= push them
back) or with less daily wearing time, keep them in place as with
1.a)/b), find alternatives there.
Alternatives
for distalization: plate appliance with screw segments
at the rear (distal screws; Y plates or Z
plates). Clasps at these segments grab the molars, and the screws
push all back 0.1 mm by 0.1 mm – in the upper as well as in the
lower jaw (compare with „cases“> Parallel
shift). After instruction, the patient can crank
the screws regularly himself. Additional clasps at the front teeth
are recommended to keep these plates with short-ranged, but high
forces well in place. Since normally not just the lastmost teeth are
to be pushed back, but many
adjacent teeth also, „cases“> „Adult treatment of
horizontal overbite“ shows how a plate appliance can be used for
this whole task, by successive modification of its numerous
triangular clasps into active springs. „Cases“> „Crozat
treatment of adult..“ shows an older-fashioned way of
single-sided successive distalization and alignment.
 2.b)
Delaire mask (face mask) frame-like
or, even more nasty but more widespread, with a vertical bar in front
of the face (see photo).
Rubber bands are stretched from there to a hook
support in the upper jaw, which is often fixed, instead of a
removable expander with likewise hooks. Frequently, expansion is done
by the profitable violence of splitting the palatal suture (4.)
before, after or parallel to the face mask treatment. The photo in
milk dentition is a 5 year old victim´s. This brutally forced
shaping of the young, growing jaws is often termed „orthopedic“,
as if comparable with the gentle effect of those well-proven
functional appliances which only re-direct the forces of the mouth
muscles to re-establish proper jaw growth.
2.b)
Delaire mask (face mask) frame-like
or, even more nasty but more widespread, with a vertical bar in front
of the face (see photo).
Rubber bands are stretched from there to a hook
support in the upper jaw, which is often fixed, instead of a
removable expander with likewise hooks. Frequently, expansion is done
by the profitable violence of splitting the palatal suture (4.)
before, after or parallel to the face mask treatment. The photo in
milk dentition is a 5 year old victim´s. This brutally forced
shaping of the young, growing jaws is often termed „orthopedic“,
as if comparable with the gentle effect of those well-proven
functional appliances which only re-direct the forces of the mouth
muscles to re-establish proper jaw growth.
Purpose:
pull the upper jaw forward. However,
3/4 of the counter force applies to the chin and
sqeezes the jaw joint permanently in back direction. The jaw joint
can take damage because it is particularly sensitive in this
direction.
 Alternatives:
several well-proven exist, e.g. in „case
examples“> „Early treatment of class III with
lightweight appliances“ and „Progenie ... mit Bimler“.
In chapter Gentle braces
B, also the maxillator (half a Bimler, but simpler) and, in
more conventional technique, bite back-shift plates. One is built
from a commercial kit for screwable back shift 0.1mm by 0.1mm, the
other is lighter, suitable in milk dentition and requires no special
parts, but is equipped with lip shields and a downward frontal
spring. Fränkel´s well-proven function regulator (FR) 3 is
further described in „Weitere Info“ subchapter „Example
of functional treatment“: its large shields transmit a similarly
strong pull (!) to the upper jaw, but not via the teeth, and the
counter force is spread in the whole mouth and not mainly onto the
jaw joints. Results of FR treatment have been proven to be very
long-term stable – if this still counts in modern orthodontics.
Alternatives:
several well-proven exist, e.g. in „case
examples“> „Early treatment of class III with
lightweight appliances“ and „Progenie ... mit Bimler“.
In chapter Gentle braces
B, also the maxillator (half a Bimler, but simpler) and, in
more conventional technique, bite back-shift plates. One is built
from a commercial kit for screwable back shift 0.1mm by 0.1mm, the
other is lighter, suitable in milk dentition and requires no special
parts, but is equipped with lip shields and a downward frontal
spring. Fränkel´s well-proven function regulator (FR) 3 is
further described in „Weitere Info“ subchapter „Example
of functional treatment“: its large shields transmit a similarly
strong pull (!) to the upper jaw, but not via the teeth, and the
counter force is spread in the whole mouth and not mainly onto the
jaw joints. Results of FR treatment have been proven to be very
long-term stable – if this still counts in modern orthodontics.
 3.a)
Herbst appliance. often fixed to all
side teeth, from molars to cuspids, by means of metal bands or
cemented plastic splints. Cleaning of these teeth is severely
hampered. As with 2.,
additional braces are often required to achieve a proper
matching of upper and lower teeth.
Since the common type of this appliance is rigid to sideward chewing
movements, proper chewing is no more possible. What means
either living on mash and porridge or risking a gastritis by
swallowing unchewed food or requiring 3-fold the time for meals. Also
any (dental care) chewing gum gets caught in this appliance. See
victims´ report below. Kinds with additional joints for
sideward movements are even more bulky,
as is also the jointless
3.a)
Herbst appliance. often fixed to all
side teeth, from molars to cuspids, by means of metal bands or
cemented plastic splints. Cleaning of these teeth is severely
hampered. As with 2.,
additional braces are often required to achieve a proper
matching of upper and lower teeth.
Since the common type of this appliance is rigid to sideward chewing
movements, proper chewing is no more possible. What means
either living on mash and porridge or risking a gastritis by
swallowing unchewed food or requiring 3-fold the time for meals. Also
any (dental care) chewing gum gets caught in this appliance. See
victims´ report below. Kinds with additional joints for
sideward movements are even more bulky,
as is also the jointless
3.b)
Functional / Fixed Mandibular
Advancer (FMA), which consists of a pair of big tenons outside
the upper molars and ramp-shaped bearings for them
outside the lower. Due to their width, this appliance is likely to
dig painfully into the cheeks.
3.c)
Jasper jumper, flex developper (smaller),
Sabbagh spring. More flexible;
nevertheless proper chewing, cleaning of teeth and mouth opening e.g.
when yawning are hampered.
Purpose a) to c): bite
jumping.
Alternatives
a) to c): as under 2.a), almost anything of Gentle
braces chapter B, in particular with „chewing
gum effect“ (including
„Weitere
Info“ subchapter Dentosophy) to
accelerate treatment of late or severe cases. If fixed braces are in
place, rubber bands can be used, or „trainers for braces“,
which would be better from the point of muscular adaptation.
 4.
fixed palatal expander (Hyrax, forced expansion,
palatal splitting, rapid palatal expansion RPE): a vice-like
appliance fixed unter the palate disrupts the palatal suture, which
is of connective tissue in children and of bone in adults. It then
makes use of a repair mechanism of our body, which generates fresh
(bone) tissue between the adjacent faces of a rupture or fracture.
After that, it is recommended to leave
the appliance for further 3 to 5 months in place, for healing
or stabilization. So, this method is not so rapid overall, see 2
victims´reports below!
4.
fixed palatal expander (Hyrax, forced expansion,
palatal splitting, rapid palatal expansion RPE): a vice-like
appliance fixed unter the palate disrupts the palatal suture, which
is of connective tissue in children and of bone in adults. It then
makes use of a repair mechanism of our body, which generates fresh
(bone) tissue between the adjacent faces of a rupture or fracture.
After that, it is recommended to leave
the appliance for further 3 to 5 months in place, for healing
or stabilization. So, this method is not so rapid overall, see 2
victims´reports below!
This
brutal method is nevertheless used for children with narrow upper jaw
as young as 4 years. Since the
palatal splitting screw is quite large in comparison to a milk
dentition, some greedy orthodontists position
it there in the plane of the teeth, so that speech is severely
hampered and every bite of food gets caught in it. A version
with plastic wings instead of metal bands facilitates the misuse of
this violent technique on milk teeth, see photo
of the 5-yr victim here. A risk study (in German) is a separate
chapter here
in the Risiken-und-Nebenwirkungen menu.
Purpose:
expansion on schedule of upper jaw to great extent.
Alternatives:
as under 1.c), but for longer time or with earlier treatment begin.
5.
pendulum appliance, distal jet: fixed little
plates with a pair of springs at the rear. „The patient (9
years) complained about speech hindrance, but the appliance worked
properly“.
Purpose: pushing the lastmost teeth
back, like purpose 2 of 2.a).
Alternatives:
see there.
6.
orthodontic implants (mini
anchorage pin, micro screw, micro-implantat anchorage MIA)
make world-wide congresses and bring profit to orthodontic
manufacturers. Courses were announced e.g. with „comparison of
products of 18 manufacturers“ (everyone wants to have a piece of
the cake, as it seems), or claimed: „600 mini pins gave no
serious trouble, but offer a quick and budget solution“ –
obviously, when compared to the cost of full braces. Alternatives
were omitted, once again, so that adults
and children are threatened with this unneccessary risk
of persistent bone inflammations,
see victims´ reports below.
Purpose:
combined with bracket braces, providing anchors for forces, or for
teeth which should themselves be used as such anchors.
Alternatives:
almost any kinds of removables, like active plates, Crozats,
Invisalign® or other splints, circumvent anchoring
problems by their rigid body. Examples are in
chapter Gentle braces A et
especially indicated under 1.a) + b) and 2.a), purpose
2.
When a covered bite is to be treated, or prolonged teeth are to
be re-introduced into the bone again, e.g. before placing a bridge,
functionals which utilize the force of biting down are especially
well-suited, including pre-fabricated trainers for many cases.
 7.
Bite Turbos and
other fixed occlusal stops which prevent biting down:
7.
Bite Turbos and
other fixed occlusal stops which prevent biting down:
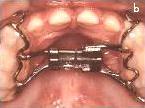
apart
from crafted fixed or removable bite plates, which require
impressions, pre-fabricated parts can be used in a surprise attack to
block the patient´s ability to chew. These are often horizontal
metal platelets which are glued to the inner faces of the incisors
(see right part of the photo). By this, chewing is rendered
impossible, worse than with a Herbst appliance (3.),
which still permits forward-backward chewing movements. Here, only
the incisors remain available to crush and mince food.
Another
method to hamper chewing is to place temporary fillings which are
much too high (see left part of the photo). In normal dentistry, this
would be severe botch-up.
Purpose: while the alignment
of crossbites or of teeth which lack occlusion may indeed be hampered
by the bite, most occlusal barriers are add-ons in multibracket
treatment of covered bite or gap closure.
Alternatives:
the bite does either not hamper treatment with removable appliances,
or they can be extended over the chewing surfaces to block it. When
screwed segments at plate appliances are used to shift teeth
laterally, e.g. for gap closure, the force is high, but is already
exhausted after just 1/10 mm. In contrast, forces of fixed braces are
of long range, but often so low that a firm matching of upper and
lower teeth can block them.
Covered bite and lacking (lateral)
occlusion can well be treated with functionals. The positioning of
the patient´s jaw in these appliances often provokes a rapid
change of jaw posture, so that a firm matching of occlusion is
loosened. This is a nice effect, which is unfortunately not obvious,
in contrast to the mode of action of brute-force methods.
In case
where brackets are already in place, pre-fabricated „trainers
for braces“, as already mentioned under 3.,
can be used to unlock occlusion. They are a special type which has
grooves for the braces.
8.
fixed spikes and tongue traps:
spikes hurt and threaten even 8-yr children, see victims´
report below. Fixed tongue traps are often prefabricated parts which
hinder speech and biting off. After their removal, the tongue
nevertheless often relapses to its old, bad habits.
Purpose:
Correction of wrong posture and function of the tongue in fixed
braces technology. Correct tongue functions are fundamental for a
healthy jaw development and to prevent relapse of corrected disorders
that have been caused by such malfunctions.
Alternatives:
Most functional appliances inherently normalize
tongue posture and motion. But also single-jaw removables can be
equipped with elements that attract the tongue. Moreover,
(speech) training can overcome the malfunctions.
------------
APPENDIX --------------
Honestly,
the following reports may be more horrible than average. But on the
other hand, they are no rare exceptions. And nobody knows before how
horrible the treatment will be, or does not plan before, how to get
out of it if it will turn out like this. Find an emergency exit at
the very end of this chapter.
Who is relying so much in good
luck elsewhere, when health and well-being are concerned? In
fact, how will suffering from such a torture affect the success in
important examinations, e.g at school?
1.a)
lingual arch, adult: big trouble, I´ve got an arch
behind my lower teeth which is fixed at the molars. Yesterday at
dinner, my tongue passed along there. At first, I felt nothing, but
when cleaning my teeth, I found a little wound under my tongue!
I
called at my orthodontist, if I could drop in, but they replied, in 4
weeks earliest...
I have eaten almost nothing today because it´s
so painful...
palatal bar (TPA), child,
age = ?: my daughter has got a TPA and can hardly eat
anything now. Is this really necessary, or can I insist on removing
it?
1.c)
Quadhelix: makes
the tongue sore, especially by eating! In each single
downbiting during the processus of chewing, the mush comes out
between the teeth at both sides, and it is the job of the tongue and
the cheeks to push it back between the teeth. Now with a
wire-skeleton-like quad helix installed under the palate, it
scratches the working tongue almost permanently, and it retains
considerable quantities of food! Chewing small things is nearly
impossible, since they get caught completely in these wires! In
France the quad helix is, apart from extractions, nowadays routinely
used for gaining space. What is done by quad
helices to 3-10 year old children, unless they are carefully
fitted, elucidates from this
report
of a quadhelix victim (20 year): “and now this wonder
gadget quad helix!
I wonder who has invented this
tool-out-of-hell. Traintracks would be a pleasure compared to this...
In the lower jaw, the crude appliance is not too nasty.... wires
prick into the tongue from below, and the bands scratch sores into
the cheeks, but the world knows greater evils!
But in the upper
jaw!!! How have they thought this should go? To explain it... a metal
bar surrounds the inner faces of the teeth, and behind the incisors
is the first source of trouble: a winding of 1 cm diameter! Disturbs
speech immensely and torments when biting off.
Yo, and now the
most evil part: beginning 2 cm behind the incisors, a metal skeleton
is under my palate that really drives me mad. It hampers my tongue to
touch the palate. A big void is held open that is really hell... any
food gets caught therein, but habitually, I want to get rid of it!
When trying to insert my tongue there, it is neatly slashed by
retained debris! Tasting and sucking and melting in the mouth is
impossible and one has to fight with the reflex of pushing every bite
of food into there!
The flux of spit is also immense, by the
tongue being at this metal cage and not at the smooth palate! Sucking
it away from there is not possible. After any meal or chocolate bar I
need to use the oral spray.
-
What am I doing at work? No oral spray there, my tongue gets slashed,
and tidying there with a piece of wire is not working well! Residues
remain everywhere – What will I do when eating elsewhere? I
cannot adapt myself to having food sticking there.
- Couldn´t
the metal be flat and in contact to the palate and allow my tongue to
contact there also?
- Can someone provide me the address of the
producer of this? I really would be keen on his explanations to this
hell instrument.“
Comment:
there are many producers, and they would say in this case that their
product had not been adapted properly.
2.a)
Two victims of headgears:
Case 1, adult:
my first night with a headgear. It drives me mad. I could rather
scratch the plaster from the walls with my bare fingers.
Where it
is hooked in, it hurts like hell, mainly on the left side. It
feels like tearing out my jaw. And it chafes in the corner of my
mouth.
During daytime, it was bearable, but not at night... I am
not a weakling, I thought...
I should wear it at least 16/24h
until next date, preferably more... and I wanted to do this for
faster progress of my treatment. But like this, I can´t stand
it ...“
Case 2 and
following, children: My
daughter has got upper and lower train tracks since 2 days, and in
addition a headgear. The pain by the train tracks was bearable, but
the head gear has really knocked her out! After wearing it for 8 hrs,
she has tremendous pain. She can´t reinsert it without tears
flowing like rivers.
So she hates it from the very start. Last
night she could not sleep with it until I gave her a painkiller at
23:30. This morning I found the headgear next to her in the bed ...
it drives her mad, and makes me a nervous wreck.
Similar pain
by a headgear was reported by a mother of a 9-yr girl: any little
movement of the head
transmitted a pain attack to the teeth where the headgear was hooked
in. After 2 days, the pain
on one side eased, but on the other side remained severe.
COMMENT:
concerning the two large teeth which are tormented like this by a
headgear, guess how many years this could reduce their lifetime!
Easing pain despite of unreduced force may signify death of tissue
around the roots. In this case, the
bone will directly connect to the tooth, so that the shock protecting
and shock absorbing function of the destroyed tissue will lack. Thus,
an increased wear of the tooth is to be expected, similar to that
which was observed on artificial teeth which were carried by
implants.
3.a)
Two victims of Herbst
appliance:
Case
1:
at the moment everything hurts and I feel
like a hamster with these thing!! I´ve got some pain pills from
my orthodontist, ...Everything hurts even if I simply try to open and
shut my mouth! I cannot think about eating today, I just drank
through a straw. [...] the first night was HORRIBLE!!! My cheeks are
completely sore and aching...my teeth are aching....and meanwhile my
jawbone is also aching!!! It is dreadful that I cannot sleep on my
side, because then it is squeezed into my cheeks, and I don´t
sleep well on the back! I´ve got 12 bands placed in total. I
don´t dare open my mouth widely, this is too painful. Cleaning
my teeth was hard this morning, takes an eternity and also hurts!! I
hope I will survive this start.... but I find these rods somewhat
nasty, and meanwhile I become aware of what you have meant with the
blocking of sideward movements! It is completely
disturbing.....(later
annex) I never get accustomed to this, it bothers all the time!
Case
2: how pupils are suffering physically and also
mentally, by the derision of their comrades:
Herbst
appliance? I had this (for 9 months). This is really nasty! They
always called me Terminator then.
... always mockery, once when I
had to give a talk in biology I nearly died .... they ran me down in
all kinds, and I heard it all, it was really like hell ... and you
look really ugly with this thing.
Some
images of Herbst appliances online show coarse screws on the lower
cuspids, which stand out by approx. 5mm. You
literally feel how they would dig holes into the flesh of your
cheeks. Nevertheless, they are boosted with
an impertinence that fools young and old patients on
certain websites as – esthetical,
- almost not hindering oral
hygiene, and
- rapid accustomization.
4.
Two victims of fixed expanders, 8 and 9 year:
Case
1: my 9-yr daughter has got this RPE
appliance since before yesterday. She can hardly eat and drink since
then. Chewing makes trouble and anything gets caught under the
appliance. Swallowing is also difficult...
Cranking the screw is
a struggle: she becomes cramped, can hardly open her mouth and
complains about aching teeth afterwards.
This was found in a
censored forum, where pain killers were recommended along with the
downright lie, that there would be no alternative to this torture.
Case 2,
8-yr, reported by her teacher:
„..the following
CITATION: >modern orthodontic treatment increasingly requires
appliances that are independent of patient compliance.<
Which
means in plain language that the patient is forced to bear and to
continue the treatment, even if she wants no more. Communication gets
replaced by compulsion.
The patient, who is often a child, can no
more take off his braces when he wants, or when his body requires it.
Well-being is much cracked up by this.
Any adult who could not
imagine this should be hampered to scratch himself when it itches.
Fixed braces are much worse than that!
Unfortunately, many
orthodentists consider just teeth, and not the whole body or the
whole person (...)
Right now I have a 8-year pupil (!) who goes
through this. Disrupting the palatal suture has taken 3 days!
Her
parents are completely unaware of what is going on with their
daughter. She is very shaky now, unconcentrated, but well-behaved.
Useless to consider speaking, it sounds like handicapped (as it is,
in fact).
From fixing of her appliance on, she draws giant, empty
faces, in which she places a tiny slanting mouth. Then she asks me if
this is beautiful and correct.
It is shocking!
I would expect
that psychical trouble will follow later, but who will then remember
her braces – „since anybody had them“?
According
to a lawyer, these are cases of bodily harm. There
is NO indication for fixed expanders in deciduous dentition or early
mixed dentition (before
the side teeth change).
Nevertheless,
the websites of several orthodontic practices show off with palatal
splitting in 3- or 4-yr young children, which had
by no means an extremely narrow jaw. The use of this most brutal
treatment is in total scorn of the powerful growth of so young
children, and of their well-being, since the size of this appliance
is almost filling out the void of their palate, so that chewing and
swallowing and speech are enormously hampered. In one example, a
child was treated first with palatal
splitting and then with a (removable) bite jumper plate, in the sense
of this sequence of fast single-task steps which was described in the
intro, insctead of using one of these well-proven removable
appliances which perform both tasks slower, but at the same time.
Even any common type of bite
jumper plate can be equipped with an expansion screw.
In
another case, two 7-yr girls had been abused for testing a new kind
of RPE appliance. Permission of this parents was acquisited by the
lie that only this procedure could create space for the wisdom teeth
later! At least one of the little test girls suffered tremendous
pain, and several had a broadened nose from it, for their whole life!
Their parents had not been warned about this side effect. The duty of
full information on medical treatment had been neglected here!
 6.
Victims of „bone piercing“ (orthodontic implants):
6.
Victims of „bone piercing“ (orthodontic implants):
Case
1, screwed in the palate: I
had been pulled two upper teeth before. Now I have some kind of
button fixed in my palate, from which wires emerge to the teeth
behind, to prevent them from being shifted. Up to now it was
bearable, but since two weeks my palate is inflammed. My ortho rinsed
it well everywhere, but nevertheless it aches more and more! Is there
no alternative? Couldn´t I wear a removable plate in addition?
What can I do to get rid of this thing and to avoid further
aggravation?
Case
2, so-called micro screws in the jaw sides: I wear
train tracks since 4 months, and I got these mini pins 1 month ago.
Under local anaesthesia, I didn´t feel the piercing, but while
screwing, she asked me often if anything hurts, which would have
signified that a tooth root is going to be damaged by the screw. One
of the screws was withdrawn and newly screwed in other position.
Then, rubber bands were stretched from the screws to the brackets.
Last saturday I discovered that my gums had overgrown one of these
rubber bands. Now I urgently need an appointment, but I´m
feared what she will do to me. My teeth are already heavily
sensitized, and also my cheeks now. Their insides are always on the
brink of bleeding, because some sharp upper wires stand rather far
out.
8.
Victims of spikes:
Spikes
were fixed in the mouth of a boy who had already been maltreated from
8 years on, first with a quad helix (1c.)
and then with unneccessary extractions. Spikes were elsewhere fixed
in the mouth of a 9-yr boy, who had been tormented with a headgear
(2a.) and a poorly-fitting
palatal bar (TPA, 1a.)
before.
Biting off and rinsing after brushing were very tedious
around the spikes. Many prick injuries made the tongue burning at any
contact with sour fruit or salad, and it was swollen for weeks. The
parents had no courage to put the offender in his place, or to use a
wire cutter to help their child at least.
In a third case, a
family dentist found spikes in the mouth of a 8-yr girl and
criticized this in a letter to the orthodontist. She replied with a
choice of international publications, which served to establish this
cruel method.
ALL
TOTAL: late sequels
4
cases at once from an abandonned forum from
2004:
CITATION:
Machoire douloureuse
j'ai porté un appareil pendant
plusieurs années: à 8 ans un appareil dentaire avec
faux palet et dés 11 ans des bagues et élastiques
pendant 4 ans. J'ai aujourd'hui 29 ans et depuis quelques mois je
ressents une douleur dans les dents, ma machoire se bloque, etc.
(...) Ma soeur qui a eu le même orthodentiste a le même
problème.
Aching jaw
I had
braces for several years: with 8 a removable plate and from 11 on
traintracks with rubber bands for 4 years. Now I´m 29, and my
teeth are aching since months, my jaw blocks etc.(...) My sister, who
was at the same orthodontist, has the same trouble.
Reply
1: Bonjour,
Votre question m' intéresse. Depuis désormais
trois ans, j'ai des problèmes de machoire (claquement,
ouverture réduite...), et il apparait de plus en plus
clairement que cela est dû à de mauvais traitements
orthodontiques, des traitements excessifs (8 dents retirées,
bagues pendant plusieurs années...). On me dit qu'il va me
falloir désormais porter jusqu'à la fin de ma vie, une
gouttière, appareil qui se porte la nuit. (...) je voudrais
savoir combien de personnes sont ainsi victimes de suites de
traitement réalisés sans discernement, par des
professionnels plus intéressés par l'argent de leurs
patients, que par leur santé...
Re:..interesting.
I suffer from jaw troubles (snapping, reduced opening...) since 3
years, and it becomes clearer now that this comes from bad or
exaggerated orthodontic treatment (8 teeth pulled, fixed braces for
several years...). Then I should wear a retainer for the rest of my
life, at night.(...) I would like to know how many people are
likewisely suffering late sequels of treatments which were mindlessly
pulled through, by experts in making money, rather than in health.
Reply
2:
traitement orthodontique raté! Ca m'est arrivé et
je ne sais pas encore ce que mes dents vont devenir enfin celles qui
me restent! Je consulte et je consulte ...mais quand je lis le nombre
d'années d'études que ces praticiens font je comprends
surtout que ça vaut le coup. Le contenu de leurs cours doit
être je pense "Comment se faire des couilles en or avec
des dents de pigeons".
Treatment
failed! Mine also, and I don´t know what the rests of my teeth
will become – of those which remained me. I pass from one doctor
to the next ... when I think about how many years these experts have
studied, I understand that it must be worth while. Curriculum maybe
„How to make a bonanza from pigeons´ teeth“.
Two
further, coupled cases from the same month elsewhere:
1.>24,
Arthrose + Arthritis im Kiefergelenk. Angebl. weil mein Biss falsch
ist (zur Info, hatte mit 14 bereits eine feste Zahnspange.) KFO sagt
feste Zahnspange würde helfen. Kosten: EUR 5900,-..<
2.>bin
20 ... Bei mir waren die Kiefergelenke/der Knorpel komplett zerstört,
konnte nichts mehr essen... Ebenfalls wegen Unterkiefer zu weit
hinten) Ich hatte im Alter von 11-14 eine feste Spange, die
allerdings nichts gebracht hat.<
1.
24 yr., arthrosis and arthritis in the jaw joints, assigned to my
wrong bite position (however, I already had fixed braces when I was
14). My new ortho recommended fixed braces again, now for 5900,-
EURO.
2. 20 yr., the cartilage in my jaw joints was completely
destroyed, I could no more eat ... also in my case the lower jaw was
standing back. I had fixed braces from 11 years to 14, but they
didn´t help anything!
3 YEARS (!) of fixed braces in
vain, despite of proper treatment age! This ortho must have been a
botcher. Order the stuff, glue the brackets and assemble with the
wire without thinking, because all will go automatically then ...
it´s so easy. And no need to care about failure and damage to
the patient, because right this provides
a fresh source of income:
2.>Therefore
I got again fixed braces with 15 years, this time from a specialist.
They weren´t removed until I was 20.<
All
in all 8 years of pain, hampered eating and hampered brushing.
Teenage youth spoiled and tooth enamel corroded, and public insurance
payed finally with our money for this over-treatment.
The
specialist seemed to have taken these 5 years to force the arches,
which had been forced by the first treatment into a uniform shape
which turned out to be highly mismatching here, into a more
appropriate shape again.
Instead of tayloring economic removables
which allow the jaws and arches to grow to a healthier shape by their
own power. Growth is normally not terminated with 15 years, see
chapters „case examples“ and Gentle
braces B.
Why aren´t treatments not
generally done with low-risk methods? Because these are less
profitable, first by themselves and second by a much lower rate of
late sequels?
Finally
instead of a happy end, here the emergency exit: go on strike
with cleaning your teeth, thus urging your ortho to dismantle
your appliance. Before, take advice of your insurance concerning
correct negotiating and financial outcome. I refuse any
responsability for any consequences here.
continue
to chapter Gentle braces
B
continue
to chapter
Gentle braces A
get
hints for searching good treatment
HOME