
Neuromuskuläre
Behandlung mit konfektionierten elastischen Hilfsmitteln, 3
Beispiele
Myofunctional
treatment with prefabricated
trainers (Angle class I, II-1, II-2, asymmetric and III)
ODF
neuro-musculaire avec des
activateurs souples sélon Soulet-Besombes, écrans
labiaux et autres moyens préfabriqués
Konfektionierte
elastische Trainingsmittel sind z.B. der
Kaukraft-Kiefer-Former,
der farbenfrohe, aber weniger
variantenreiche Positionstrainer (Foto links und Mundfoto), der
Face Former nach Berndsen (Unna) oder die Mundvorhofplatte, die
es aus starrem oder elastischem Material gibt. Neuromuskulär
bedeutet, dass sie im Mund Reize ausüben, die
Reaktionen der Muskeln hervorrufen, die der Selbstregulation
unterliegen.

Da
diese Geräte beide Kiefer umfassen, werden die Regelkreise der
verschiedenen Kaumuskeln angesprochen, deren Kräfte
beträchtlich sind. Die Geräte sind so geformt, dass sie
diese Kräfte in Richtung auf eine gesunde Gebissentwicklung
umlenken, und dass muskuläre Fehlfunktionen normalisiert
werden.
Wegen dieser kräftigen Reiz-Reaktions-Wirkung
(„Kaugummieffekt“) genügt es dabei für eine
effektive Behandlung, anders als beim Bionator oder Crozat-Gerät,
sie nachts und 1 Stunde am Tag zu tragen.
Wie mit anderen,
teureren Mitteln zeigen auch hier Frühbehandlungen die
schnellsten Erfolge. Jedoch kann diese Umnutzung der Kaumuskelkräfte
auch in die Fehlstellungen von Spätfällen noch Bewegung
bringen, und durch die moderaten Tragezeit-Anforderungen eignet sich
die neuromuskuläre Behandlung auch für
Vollzeit-Berufstätige und Ganztagsschüler.

Der
1. Beispielpatient ist fast 9 Jahre und hat im frühen
Wechselgebiss eine enge Deckbiss-Front (Angle Klasse II-2) in
Entwicklung.
Im Mundfoto ist der Unterkiefer vorgeschoben, um auch
die untere Enge zu zeigen. Der Milch-2er geht oben nicht auf Lücke,
und sein Nachfolger zeichnet sich als Vorwölbung ab.
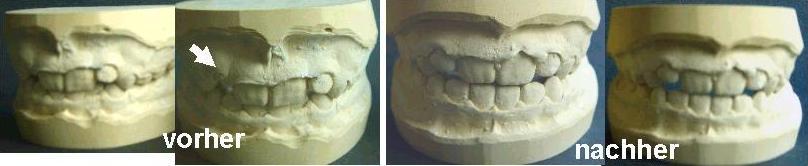
Im
Anfangs-Gipsmodell 1 Monat später tritt er ebenso hochstehend
wie sein Gegenpart aus, und im Zusammenbiss ist eine
Tiefbiss-Situation auch im Seitenzahnbereich zu erkennen (muskuläres
Ungleichgewicht).
Nach 10 Monaten Behandlung, hier mit dem
Positionstrainer, hat sich der 22 weitgehend eingereiht, und der 12
ist auf gutem Wege dahin. Die unteren Frontzähne stehen nun
engstandsfrei, und in der Vertikalen ist der Tiefbiss behoben und
eine gesicherte Seitenverzahnung erreicht. Offenbar hat der
Trainer auch unten die Breitenentwicklung gefördert. Die
3-dimensionale Wirkung dieser einfachen Behandlungsmethode wird
ersichtlich.
Die Schneidezähne zeigen jetzt knappen
Überbiss, haben aber noch nicht ihre volle Länge erreicht.
Zur Sicherung und weiteren Besserung sollte der Trainer, oder ggf.
seine nächste Größe, nachts weiter getragen werden.
Dass
ein Deckbiss in Entwicklung noch mit einfachen Mitteln heilbar ist,
während er im bleibenden Gebiss als hartnäckig gilt, deckt
sich mit den Beobachtungen von Bimler. Zur Deckbiss-Behandlung im
Wechselgebiss empfahl er das Standardgerät (Bimler-A), während
das anspruchsvollere Deckbiss-Gerät (Bimler-B) für
Spätfälle konzipiert war. Ansonsten wird noch viel mehr
Aufwand und Belastung mit Deckbisspatienten im bleibenden Gebiss
getrieben, wie z.B. feste Biss-Sperren.
Ähnlich hilfreich ist
die Frühbehandlung für Patienten mit Progenie oder
Schmalkiefer. Hier stehen als einfache Behandlungsmittel
entsprechende Typen des Kaukraft Kiefer-Formers zur Verfügung.
Prefabricated
training appliances out of elastic materials are for example the
Muscle
force jaw shaper,
colourful pre-orthodontic trainers (uppermost photos) e.g. of John
Flutter, Australia www.jfdental.com,
which have no special types for
expansion, and prefabricated lip shields of
various sources. Myofunctional
means that they stimulate muscular activity in the
mouth, which is under nervous control of the patient.
Since these
appliances comprise both jaws, the feedback circuits of the strong
chewing muscles are addressed, and the appliances are designed such
that they re-direct these forces for a proper development of the jaws
and dentition, and normalize malfunctions of the oral muscles.
Due
to this strong feedback effect („chewing gum effect“),
night time and just 1 hour of daytime wear is sufficient for
effective treatment, in contrast to the requirements of rigid
appliances, e.g. activators or Crozat.
As well as for other, more
expensive therapies, early („interceptive“) treatment gives
the fastest success. But this re-direction of chewing forces can also
help to improve the positions of crooked teeth and the shape of the
dental arches in late cases, and the moderate daily wearing time
makes myofunctional orthodontics also
suitable for full-time workers or -pupils.
An
almost 9-yr patient gives the 1. example here.
In early mixed dentition, he has crowded teeth and a covered
bite (Angle class II,2) in development.
In the mouth photo, the
lower jaw is shifted forward, to reveal also the lower crowding. The
remaining upper milk incisor has no spacing yet, and its successor
swells the gum.
In
the plaster casts at start of treatment 1 month later, this tooth
starts to stick out as its counterpart. The occlusion shows a deep
bite, even on the sides, which indicates a muscular inequilibrium.
After 10 month of treatment with a position trainer, the earlier
lateral incisor has almost lined up, and the later one is growing in
quite well. The lower incisors have well aligned, and in vertical
direction, the deep bite is released, and a healthy occlusion has
developped. Obviously, the trainer has also increased the lower
arch width. The 3-dimensional effect of this inexpensive appliance
can be seen here.
The incisors are now hardly overlapping,
but have not yet reached their full length. Night time wear of the
trainer, or of its next size, should be continued to maintain and
further improve the obtained result.
Whereas
a covered bite in adult dentition is persistent, Bimler had also
observed that it can be cured by simpler means as long as it is in
state of development. Of his appliances which also use the chewing
gum effect, he recommended the A or standard type for early, and the
more sophisticated B type for late treatment of covered bite. Such
patients experience elsewhere much more expense and burden, e.g.
fixed bite blockers.
Early treatment is also advised in case
of progenic bite ( Angle class III) or of narrow upper jaw.
Special types of the Muscle force jaw-shaper are available for these
tasks.

Les
appareils préfabriqués pour l´ODF
neuro-musculaire sont
par ex. les
Gouttières
d´Harmonisation Fonctionelle
ou les activateurs pluri-fonctionnels de www.sodis-apf.fr,
ainsi que les écrans labiaux préfabriqués.
Neuro-musculaire
signifie que ces dispositifs stimulent
l´activité de la musculature buccale,
qui est sous contrôle du patient.
Car
l´appareil comprend les deux mâchoires ici, il adresse
les muscles masticatoires et ses circuits régulateurs.
L´appareil est construit tellement qu´il dévie ces
forces considérables vers la développement sain de la
dentition, et qu´il normalise les fonctions atypiques de la
musculature buccale.
Renforcé
par cet soi-disant „effet
de chewing gum“, un temps de port nocturne et
d´une heure pendant la journée seulement
suffirait pour le progrès du
traitement, pendant que les appareils rigides en nécessitent
davantage.
Ici
comme pour autres thérapies plus coûteuses, les
traitements précoces donnent les résultats au plus
vite. Mais cette utilisation des forces masticatoires peut même
améliorer les dysgnathies en cas tardifs. En plus, le temps
modéré de port quotidien fait l´orthopédie
neuro-musculaire accessible même aux travailleurs ou élèves
de plein temps.
Le
patient du 1. exemple a presque 9 ans et une
dentition mixte précoce avec encombrement
et recouvrement (classe II,2) en voie de développement.
Il a avancé sa mâchoire pour la photo orale, pour
montrer l´encombrement inférieur. L´incisive de
lait qui reste en haut n´a pas encore des intervalles, et sa
dent successeuse gonfle la gencive au dessus.
Dans les modèles
en plâtre au debut du traitement 1 mois plus tard, cette dent
pousse trop haut, de même façon que son pendant.
L´occlusion est trop profonde même aux côtés,
ce qui indique un inéquilibre musculaire.
Après 10
mois de traitement avec un position trainer, cette première
incisive latérale s´est bien alignée, et l´autre
pousse déjà assez bien au correct endroit. Les
incisives inférieures se sont bien alignées, et en
direction verticale, le recouvrement est soulagé, et une
occlusion saine s´est établi. Apparemment, la
gouttière à aussi stimulé le développement
transversal de l´arcade inférieure. L´effet
3-dimensional de cet moyen peu coûteux se voit bien
ici.
Ensuite,
les incisives se recouvrent peu, mais leur croissance n´est pas
encore fini. Pour garder et améliorer le résultat, la
gouttière, ou sa taille suivante, devrait encore être
portée au nuit.
Un
recouvrement en dentition définitive est en général
persistant, mais Bimler a aussi observé
qu´en dentition
mixte, cette dysgnathie peut être guéri sans moyens
spéciaux. Parmi ses appareils qui aussi utilisent l´effet
de chewing-gum, il recommande le type A
(standard) pour le traitement précoce et le type B, qui est
plus difficile, pour le traitement tardif du recouvrement.
Ailleurs, ces patients sont soumises de grand renfort et peine, par
ex. des multibaques avec des additifs aussi
fixes, qui bloquent la mastication.
Le traitement
précoce est pareillement conseillé en cas de
progénie (classe III) ou en cas de maxillaire étroite.
Types spéciaux de la Gouttière
d´Harmonisation Fonctionelle ou des autres activateurs souples
sont
disponibles pour ces tâches.
Das
2. Beispiel zeigt, wie Kaukraft Kiefer-Former bei den häufigeren
Rückbisslagen der Angle-Klasse II-1 helfen.
Die gezeigten
Zwischenmodelle wurden nach 9-monatiger Anwendung eines
Standard-Formers genommen. Sie lassen sich noch in der alten
Rückbisslage zusammensetzen, aber auch schon in Normalbisslage.
Für sie fällt der Oberkiefer jedoch etwas schmal aus.
Schließlich hatte er sich bisher zusammen mit dem rückliegenden
Unterkiefer entwickelt. Weil diese Konstellation öfters
vorkommt, sind für ihre Behandlung mit Aktivatoren
3-Teiler-Aktivatorenschrauben im Handel, während Dehnschrauben
an Vorschubdoppelplatten (VDP) sowieso oben und unten unabhängig
sind.
Im Beispiel wurde die Behandlung daher mit einem
Schmalkiefer-Former fortgesetzt. Um dabei die Spitzfront weiter zu
normalisieren, die anfangs sicherlich ausgeprägter war, wurde
für diesen Former zudem ein härteres Material gewählt.
 The
2. example shows, how Muscle
force jaw-shapers can help against the frequent overjets of the
Angle class II,1 type.
The
2. example shows, how Muscle
force jaw-shapers can help against the frequent overjets of the
Angle class II,1 type.
The
plaster models here have been taken after wearing a standard
jaw shaper for 9 months. They can still be assembled in the former
backward position of the lower jaw, but also in normal occlusion
already. For this, however, the upper jaw has not yet enough width,
since it had formerly grown in accordance to the back-lying lower
jaw. A little width still lacks, and for this quite frequent
syndrome, special expansion screws are available for activators,
which expand only their upper half. In double plate appliances, on
the other hand, upper and lower plate can be expanded independently.
But here, treatment is
continued with a jaw shaper of the narrow jaw type, and a harder
material is chosen for it, to further normalize the positions of the
central incisors.
Le
2. exemple montre comme
l´activateur souple aide aux décalages maxillaires de la
classe II,1, qui sont assez fréquents.
Les
moulages ont été prises après 9 mois de
traitement avec un activateur souple de type standard. On peut les
toujours joindre en occlusion décalante, mais aussi déjà
en occlusion normale. Pour cela, cependant, la mâchoire
supérieure est toujours un peu étroite, car auparavant,
elle s´était développée à mesure de
la mâchoire inférieure qui était trop en arrière.
Des vérins spéciaux existent pour traiter ce syndrome
avec un activateur rigide 3-sectionné, pendant que les
propulseurs à plaques-doubles peuvent être équipés
avec des vérins standard pour l´expansion indépendante
en haut et en bas.
L´exemple
ici est continué avec une gouttière d´harmonisation
fonctionelle de type pour la maxillaire étroite, et en
matériau moins élastique, pour mieux continuer
l´alignement des incisives centrales.

Fehlentwicklungen
früh erkennen und auffangen:
Im 3. Beispiel würde
der 7-Jährige unbehandelt nicht nur Engstand, sondern auch einen
Schiefbiss durch Kieferschwenkung entwickeln. Dieser ist im
Frontal-Foto kaum zu sehen, weil er sich in einer ungleichen
Längs-Verzahnung beider Kieferseiten äußert, meist
eine im Neutralbiss und die andere im Distalbiss
(Rücklage-Verzahnung).
Er ist abzugrenzen von einer
sogenannten dentalen Mittellinien-Verschiebung, bei der Schneidezähne
in vorzeitige Lücken übergewandert sind, aber die
Seitenverzahnung symmetrisch bleibt, und von einem Schiefbiss durch
reine Seitverschiebung des Unterkiefers, die sich als einseitiger
Kreuzbiss zeigt, als Ausweich-Reaktion auf einen relativ zu schmalen
Oberkiefer entsteht und im Frühstadium mit einer schlichten
Oberkiefer-“Dehnung“ behebbar ist (Dehnplatte, Crozat,
Schmalkiefer-Former, ..).
Fälle mit seitlichem Kreuzbiss
finden sich hier im Unterkapitel Nichtanlagen (die älteren
Patienten dort).
Im
Unterkapitel Mittenkorrektur wird eine dentale
Mittellinien-Verschiebung behoben, während man diese
Überwanderung zur minimalen Behandlung einer einseitigen
Nichtanlage-Lücke als natürliche Lückenschluss-Tendenz
zulassen und fördern könnte.
im Unterkapitel
Erwachsenenbehandlung,
Engstände liegt beim
3. Patienten eine volle Kieferschwenkung vor, an der nicht mehr
gerührt wird, weil sich die Knochen und Gelenke seit langem
daran angepasst haben. Trotzdem konnte hier die Frontzahn-Ästhetik
mit geringem Aufwand verbessert werden.
Im
Sinne einer präventiven Kieferorthopädie bekam hier
der 7-Jährige sogleich einen Positionstrainer (Frühbehandlung),
womit nach 1 Jahr eine deutliche Besserung erzielt war, aber die
Anschlussgröße fehlte, so dass 1 Jahr ohne Behandlung
folgte. Dies ergibt die +2,0 Jahre in den Fotos: die Schneidezähne
stehen engstandsfrei, aber rechtsseitig besteht 1 volle
Prämolarenbreite Rücklage-Verzahnung (linke Seite nicht
gezeigt, da normal).

Bis
zu den nächsten Gipsmodellen wurde 12 Monate mit dem
nächstgrößeren Positionstrainer fortgesetzt: die
Kieferschwenkung ging auf 1/2 Prämolarenbreite (Längs-Kopfbiss)
zurück, die Kieferbreite nahm um 1,5 mm zu, Seitenzähne
beginnen zu wechseln und der Trainer hilft, sie engstandsfrei
einzureihen.
Die Behandlung wäre mit einer Folgegröße
fortzusetzen, aber zeigt, dass konfektionierte Trainer ein schonendes
und wirtschaftliches Mittel sein können, um einer abwegigen
Gebissentwicklung zuvor zu kommen. Sie führen nicht nur die
Zahnbögen in Idealrillen, sondern auch alle Zähne in eine
Ebene und die Kiefer in eine gesunde Bisslage. So können sie
nicht nur eine Zunahme von Fehlstellungen stoppen, sondern auch
Fehlentwicklungen normalisieren.
Dennoch war die Frühbehandlung
hier keine Kassenleistung. Das normale Behandlungsalter abzuwarten,
hätte die Aufgaben jedoch erschwert und an sanften Mitteln
FKO-Geräte mit verstellbarer Biss-Führung gebraucht, wie
z.B. Bimler, U-Bügel-Aktivatoren oder Pro-Stab-Platten.
Trace
and treat deviations early:
In the 3. example,
the 7-yr patient would untreated not just develop crowding, but
moreover an asymmetric occlusion by swivel of the lower jaw.
This is hardly seen in the frontal image, and is to distinguish from
a dental shift of the midline, where the incisors had migrated into a
premature gap, and from a pure lateral shift of the lower jaw, to
evade a too narrow upper jaw. This latter manifests in a single-sided
crossbite and can be treated easily, as long as in early stage, by a
simple upper expansion (plate expander, crozat, specialized trainers
for narrow upper jaw, ..).
Cases
with a lateral crossbite are included in the sub-chapter Lack
of 2s or 5s (the older patients
there). A midline deviation is treated in sub-chapter Mid-line
correction. On the contrary, such a dental migration should be
permitted and enhanced for a minimal treatment of a lacking lateral
incisor, in the sense of a natural solution.
A
true and full swivel of the jaw is found in the 3. patient of
sub-chapter Adult treatment of crowding. It
is left untreated there, since bone and joints had adapted to it long
time ago. Nevertheless, the crowded teeth were aligned there by means
of rather inexpensive plate appliances.
In
the sense of prophylactic treatment, the 7-yr boy here
received a position trainer. This achieved quite a good improvement
during 1 year, before it became too small. Since the next size was
still too large, 1 untreated year followed and gave the plaster
models „+2.0 Jahre“: the incisors are no more crowded, but
the right side has still a full distal occlusion (the left side is
not shown, because normal).
Now, the next size of the position
trainer could be worn, and in the next plaster models after 12
months, the single-sided distal occlusion is reduced by half. The
jaws gained 1,5 mm in width, side teeth start to change and the
trainer prevents them from growing false.
This treatment is to be
continued, if required with a trainer of subsequent size, but 3
trainers would still be a gentle and economic means to prevent odd
jaw growth and crooked teeth. They guide the dental arches into
grooves of anatomic shape, all teeth into plane and the jaws in a
proper occlusion. In contrast, postponing the treatment here would
have rendered it much more tedious and expensive, e.g. with
adjustable functional appliances as gentle means: Bimler, U-bow
activators, plates with single-sided bite jumper, ...

Détecter
et traiter les malocclusions en voie de développement:
Au
3. exemple, le patient de 7 ans
est en voie de développer un encombrement
des incisives et en plus, la mâchoire inférieure est
pivotée dans une malocclusion asymétrique (qui
se voit guère à la photo frontale). Celle-ci est
à discerner d´un déplacement de la ligne médiane,
qui vient d´une migration des dents vers une lacune précoce,
et d´un déplacement latéral de la
mâchoire inférieure dans un articulé inversé
latéral, qui vient
souvent d´une étroitesse de la mâchoire
supérieure. Elle se traite facilement au stade précoce
par l´expansion en plaque, en bimler, en
activateur souple ...
Les
cas cliniques avec un articulé
inversé latéral sont compris au sous-chapitre
Agénesie (les aînés là).
La ligne médiane est corrigée au sous-chapitre
correspondant, mais sa déviation peut être permis, et la
migration dentaire soutenue, en cas d´une ágenesie d´une
incisive latérale.
Une
máchoire pivotée se trouve au 3. cas du sous-chapitre
Traitement
d´encombrement / chevauchement adulte,
et n´êtait plus traitée là, car les os et
articulations s´y sont adaptés depuis longtemps.
Cependant, les incisives encombrées étaient bien
alignées par moyen des plaques peu coûteuses.
Au
sens de l´ODF préventive ici, le garçon de
7 ans recevait un activateur souple. Ceci améliorait la
situation pendant une année, et puis devenait trop petit. Car
la taille suivante de cette sorte était toujours trop grande,
une année sans traitement suivait. Ensuite, les modèles
en plâtre „+2.0 Jahre“ montrent les incisives
alignées, mais le côté droite est toujours en
malocclusion distale (le gauche n´est pas montré, car
normale).
Maintenant,
l´activateur de la taille suivante était juste, et après
12 mois, les modèles en plâtre suivants montrent que la
malocclusion unilatérale était réduite à
moitié. Les mâchoires s´étaient élargis
par 1,5 mm, quelques dents définitives paraissent déjà
aux côtés et séraient alignées dans
l´activateur.
Ce
cas sérait à continuer avec cet activateur ou avec sa
taille suivante, mais même 3 activateurs préfabriqués
séraient toujours un moyen économique et doux à
prévenir le développement des malocclusions ou des
dents chevauchantes. Ils guident les arcades dans les raies en forme
anatomique, toutes les dents au niveau et les mâchoires dans
l´occlusion saine. Par contre, un délai du traitement
l´aurait fait ici beaucoup
plus pénible et onéreux. Quelques appareils fonctionels
réglables contre la máchoire
pivotée séraient les Bimler ou les double-plaques
(plaques à propulseur unilatéral,
activateurs
jumelés par anse „U“, kinéteurs de
Stockfisch, ..).
Quellen
sources: Dr. Brigitte
Krause-Kulla, Turmstr.
35, 06110 Halle (Saale),
Tel. 0345 1200382, oder
06188 Niemberg, Tel. 034604 20208
zurück
back retour
Letztes
Update dieses Teils +++ last
update +++ dernière
mise à jour: 29.08.2011